Improving Patient Safety in Surgical Care
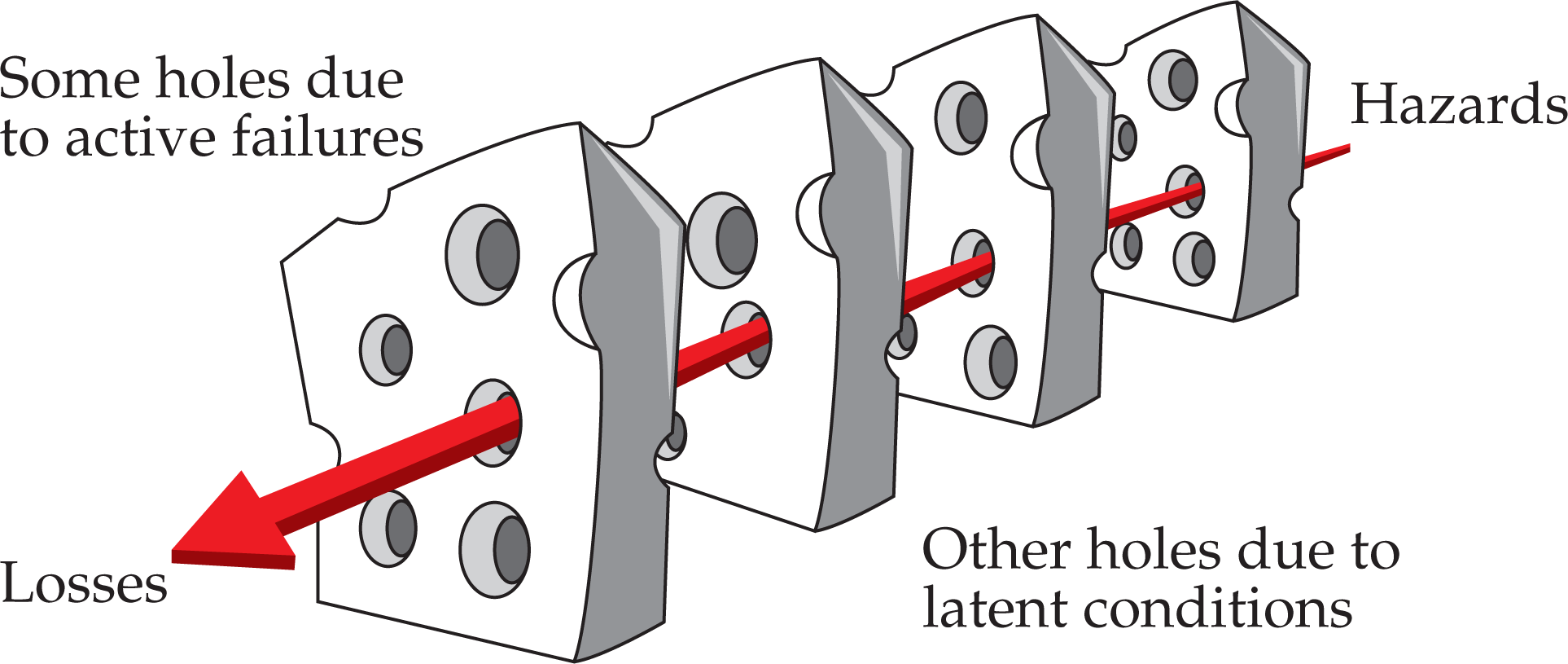
- Use of sophisticated nonmedical systems approaches to improving surgical patient safety
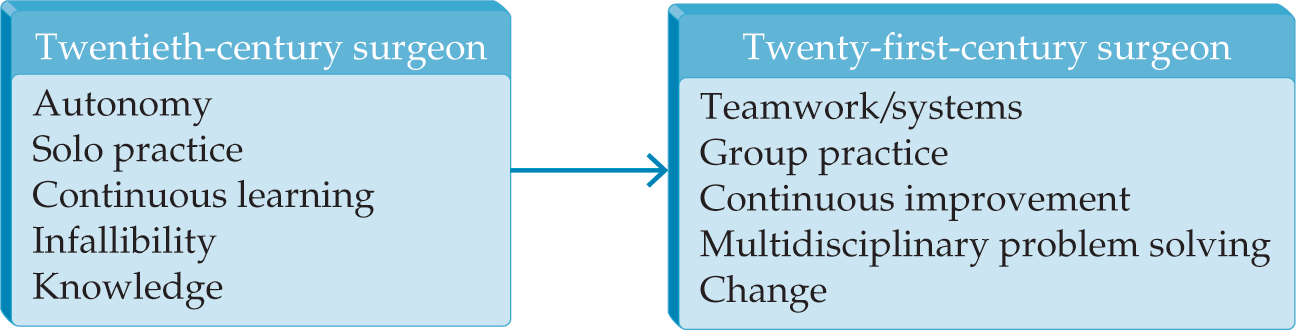
- Recognition and implementation of standardization across surgical practices and integrated health systems to improve surgical patient safety
- National programs aimed at developing grassroots efforts to improve surgical safety at the individual, practice, and health system levels